PREPARED BY
Dr Afraz Sherazi
Plastic & reconstructive surgery

Burn is a coagulation necrosis of the skin and underlying tissues due to wide range of temperature ranging from the lowest (frostbite) to the highest( electrical injury).
- Burns is a type of coagulative necrosis caused by heat, transferred from the source to the body.
- Frostbite which occurs in cold countries is also a coagulative necrosis but it is caused by extreme degrees of cold.
- A burn is one of the most serious injuries that can be inflicted on the body.
- Burns never occur at temperatures less than 44°C
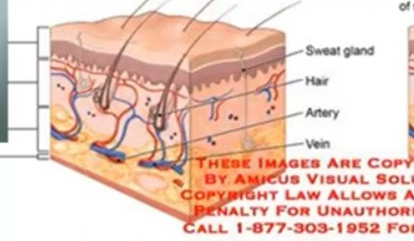
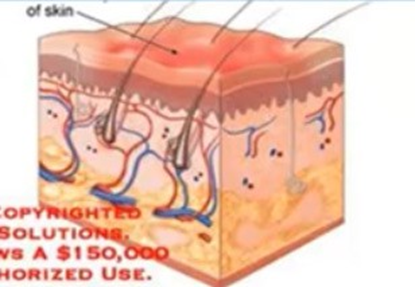
Functions of the Skin:
- It forms a barrier against invasion by micro-organisms.
- It prevents excessive loss of water from the body.
- It helps in the regulation of body temperature by secretion of sweat.
- Sensory receptors in the skin protect the body from injurious insults.
- Formation of vitamin D

CAUSES OF BURN
•1-Thermal burn : most common cause which may be caused by
•Scalds: are caused by boiled liquids; they often affect children.
Flame burns: Affect any age, the most common burn industrial accident.
Contact burns due to direct contact with hot objects (e.g. irons).
Flash burns: are caused by explosion of natural gas or other flammable liquid
•2-Chemical burn :
•Alkalis (cause a liquefactive necrosis) Alkalis produce more tissue destruction than acids
•Acids (cause a coagulative necrosis)
•Organic compounds
•Phosphorus
•3-Electrical burn :
•Low voltage <1,000 V
•High voltage >1,000 V
•4-Radiation injury
Classification of burns
- According to the extent (in relation to total body surface “TBSA” )
- A major burn: More than 30 % of the body surface area.
- An intermediate burn:
- 15 – 30% in adults.
- 10 – 30% in children.
- A minor burn:
- Less than 15% in adults.
Less than 10% in children
Body response to burn
1 Local response:
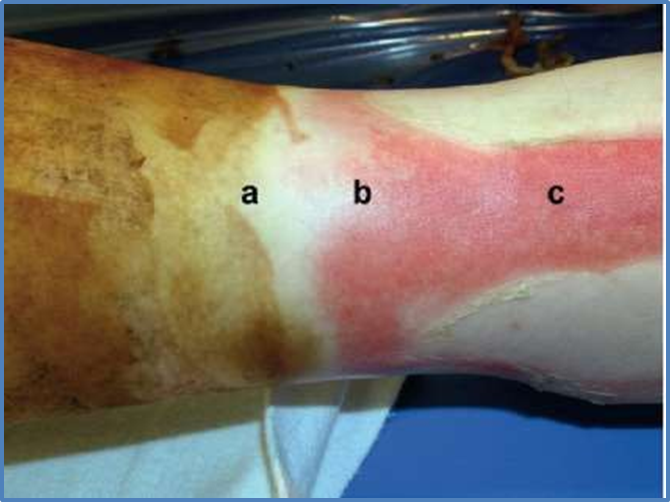
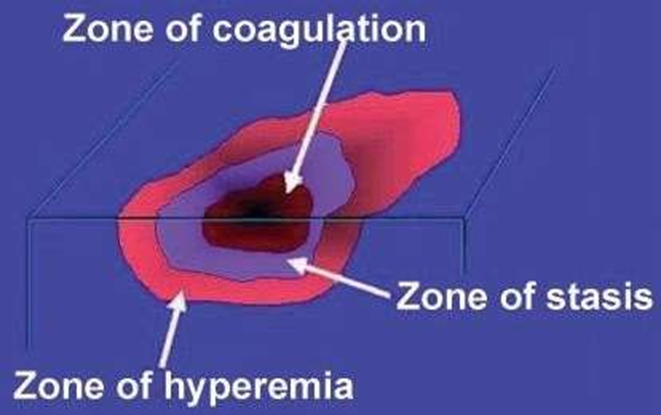
The three zones of a burn were described by Jackson in 1947.
a .Zone of coagulation (necrosis).
b .Zone of stasis (edema) .
c. Zone of hyperemia (inflammation) .

2-Systemic response:
Release of cytokines and other inflammatory mediators at the site of injury has a systemic effect once the burn reaches 30% of total body surface area.
- Cardiovascular changes—Capillary permeability is increased→ loss of intravascular proteins and fluids into the interstitial compartment→edema. Peripheral and splanchnic vasoconstriction occurs. Myocardial contractility is decreased,possibly due to release of tumour necrosis factor . These changes, coupled with fluid loss from the burn wound, result in systemic hypotension and end organ hypoperfusion.
- Respiratorychanges—Inflammatory mediators cause bronchoconstriction , and in
severe burns adult respiratory distress syndrome can occur.
- Metabolicchanges—The basal metabolic rate increases up to three times its original rate. This, coupled with splanchnic hypoperfusion, necessitates early and aggressive enteral feeding to decrease catabolism and maintain gut integrity.
- Immunological changes—Non-specific down regulation of the immune response occurs, affecting both cell mediated and humoral pathways.
Hematologic—There is immediate red blood cell destruction in direct proportion to the extent of the burn, particularly third-degree burns. Endothelial injury may lead to release of thromboplastins and to collagen exposure; the latter then initiates platelet adhesion, aggregation, and contact activation of factor XII. Severe full- thickness burns induce consumption of coagulation factors at the burn site, which contributes to the (DIC).
Gastrointestinal—Ileus is universal in patients with burns of more than 25% total body surface area (TBSA). Gastric a n d duodenal mucosal damage, secondary to focal ischemia, can be observed as early as 3–5 h postburn. If the mucosa is unprotected, the early erosions may progress to frank ulceration.
▣ Endocrine—In the early postburn period, a catabolic endocrine pattern develops that is characterized by elevated glucagon, cortisol, and catecholamine levels with depressed insulin and triiodothyronine
levels→ negative nitrogen balance. Their magnitude correlates with the size of the burn area.
- Without intervention, patients with serious burns die for three primary reasons. Burn shock in the first day, respiratory failure in the following 3–5 days, and burn wound sepsis in subsequent weeks.
- The initial management of a severely burnt patient is similar to that of any trauma patient. A modified “advanced trauma life support” primary survey is performed, with particular emphasis on assessment of the airway and breathing. The burn injury must not distract from this sequential assessment, otherwise serious associated injuries may be missed.
- The survival should not be the only goal of the management.
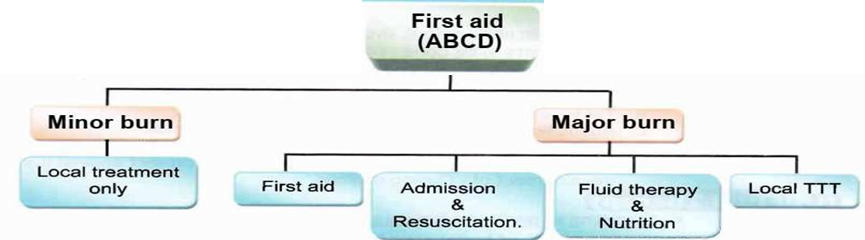
- hospital admission

- Second and third degree burns greater than 10% TBSA in patients younger than 10 years and older than 50 years.
- Second and third degree burns greater than 20%.
- Third degree burns greater than 5%.
- Burns to face, hands, feet, genitalia, perineum and major joints.
- Electrical burns (including lightning injury).
- Chemical burns.
- Inhalation injury.
- Patients with pre-existing conditions.
- Circumferential third degree burns to extremity or chest.
- Burns with concomitant trauma with a great risk of morbidity and mortality (i.e. explosion trauma).
2. Initial care: (ABCDEF):
A:AIRWAY: Endotracheal intubations is indicated if patient ( Semicomatose, Deep burn to face and neck and any suspicion of inhalational injury).
Intubaton should done early
When intubation is difficult, tracheostomy should be done.
Give 100% O2 if there is suspicion of inhalational injury Assess movement of chest wall to exclude restricted movement due to eschar.
C=circulation:
Assess peripheral perfusion
ECG monitoring in case of electrical injury Stop bleeding if associated with vascular injury
Initially should established good I.V line, if not possible
→Venous cutdown
Assess neurological status
Note any gross deformity (fracture)
E=exposure:
Expose all body to exclude other trauma and to evaluate the burn wound.
Avoid hypothermia
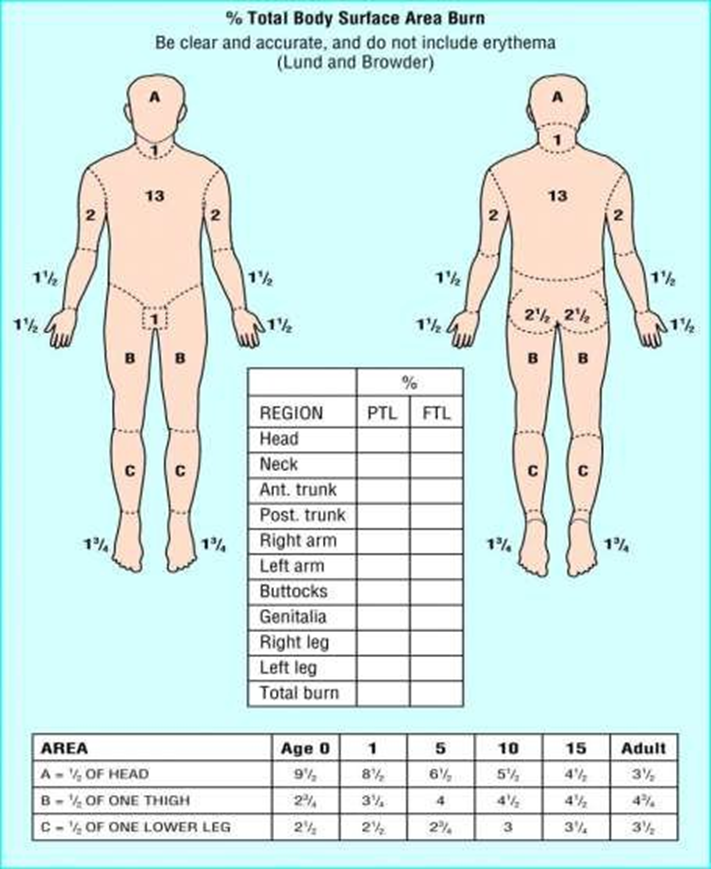
1 Assessment of burn surface area by:
- Lund and Browder chart.
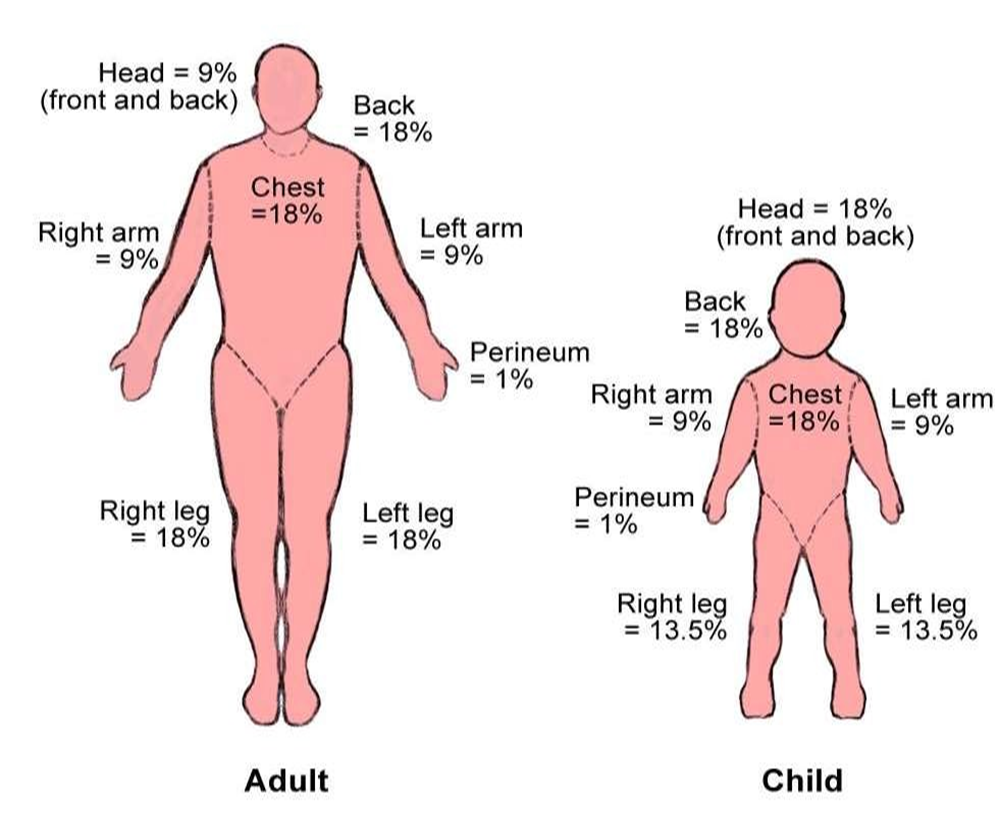
- Wallace rule of nines.
- Palmar surface—The surface area of a patient’s palm (including fingers) is roughly 0.8 – 1% of total body surface area.
2-Assessment of burn depth by clinical examination.

·TBSA is estimated by:
Rule of 9: This method is easy but not accurate in children due to large size of the head in relation to the rest of the body


• What is the importance of calculating surface area of burn?
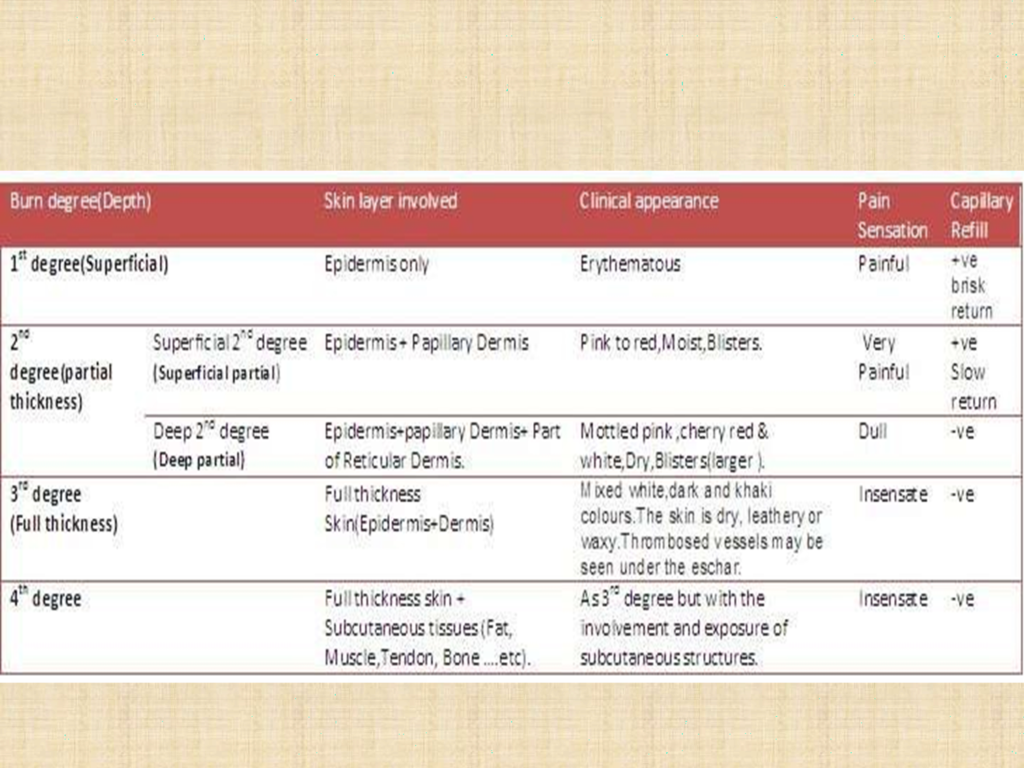

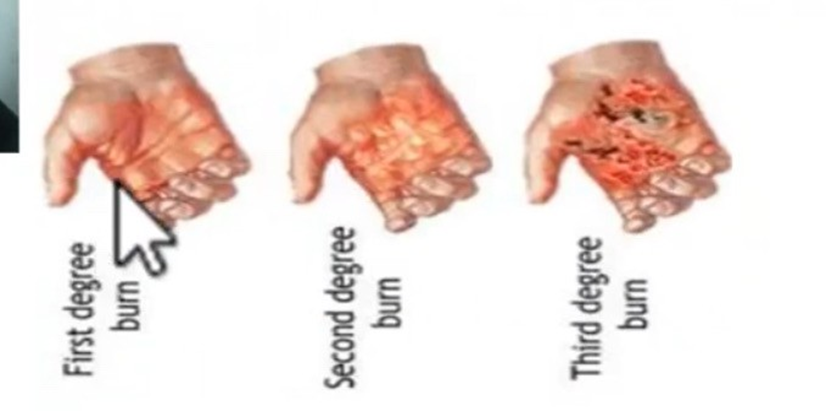
First degree: Here the epidermis looks red and painful, no blisters, heals rapidly in 5–7 days by epithelialisation without scarring. It shows capillary filling


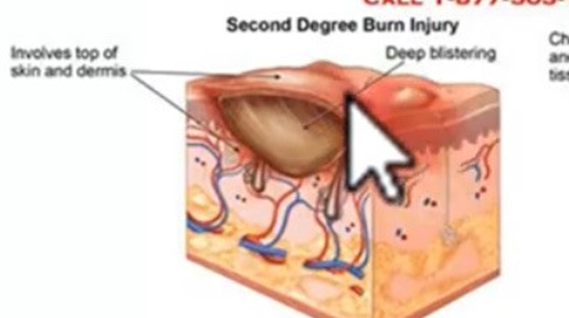
2nd degree(partial thickness)
Second degree: The affected area is mottled, red, painful, with blisters, heals by epithelialisation in 14–21 days.
(Superficial partial) Superficial second degree burn heals, causing pigmentation

(Deep partial) burn heals, causing scarring, and pigmentation

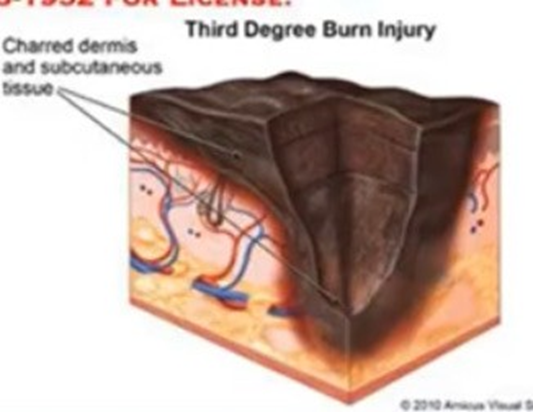
Third degree: The affected area is charred, parchment like, painless and insensitive, with thrombosis of superficial vessels. These wound must heal by re-epithelialisation from wound edge. It requires grafting


Fourth degree: Involves the underlying tissues—muscles, bone

Complications of Burns:
Systemic complications:
Shock:
| Immediate | Early | Late |
| Neurogenic from severity of pain | Hypovolemic due to under correction of lost fluid | after 1 week from infection |
- In Burn above 15% of surface area, the loss of fluid produces shock
Pulmonary complications:
| Immediate | Early | Late |
| Asphyxia Due to inhalation injury | Pneumothorax Pneumonia Pulmonary embolism | Respiratory failure type II Hypoxia, hypercapnia (ARDS) |
Cardiovascular complications:
- Acute left ventricular failure
- Congestive heart failure
- Arrhythmia (especially in electrical burn).
- Myocardial infarction (either due to stress or hypovolemia & ↑ viscosity).
Renal complications:
- Acute tubular necrosis (acute cortical necrosis) due to release of cytokines & ILs.
- Myoglobinuria & hemoglobinuria (especially with electrical burn).
- ARF (due to hypovolemic shock→ leading to water & electrolyte imbalance.
Gastrointestinal complications:
- Adynamic ileus: Acute gastric dilatation due to severe sympathetic stimulation & release of cytokines & ILs. Usually occurs early and may necessitate the insertion of a nasogastric tube.
- Curling’s Ulcer: due to stress → splanchnic vasoconstriction→ Ischemia→ destruction of mucosa.
- Liver dysfunction: due to ischemia & toxins.
- Recently acute ulceration of the colon may occur and it is suggested to be due to fungal infection
- Multiorgan failure: Often follows pulmonary insufficiency or sepsis → death.
Psychological complications.
- Septic complications:
- Urinary tract infection.
- Burn wound sepsis.
- Pneumonia.
- Septic shock.
- Septic thrombophlebitis
Endocrine system complications:
- ↑ Catecholamines from stress.
- ↑ Cortisol and ADH → Na & H2O retention.
- ↑ Protein catabolism → -ve nitrogen balance
Local complications:
- Early local complications:
- Infection:
- The primary cause of death in burnt patients due to immunosuppression.
- It occurs usually between 4-7 days post-burn.
- It may be bacterial, viral or fungal.
- It may be either exogenous or endogenous sources.
- Infection may lead to the development of septicaemia and septic shock.
- Treatment by proper local burn wound care
- The value of systemic antibiotics in the prevention of infection is doubtful.
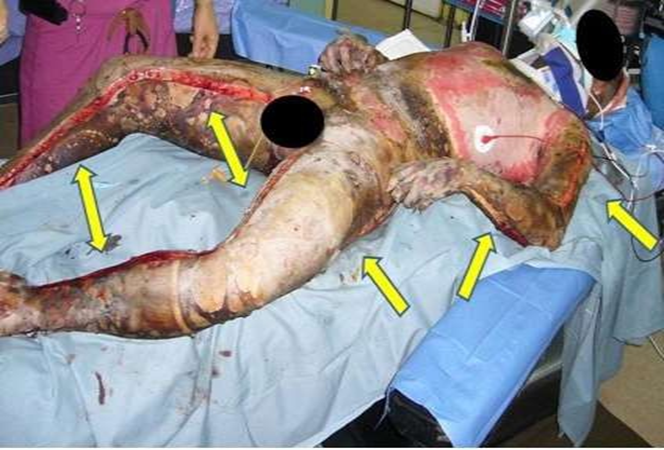
- Constricting eschars: In deep circumferential burns
- Infection:
- On chest → dyspnoea due to restriction of chest expansion.
- On limbs → limbs ischaemia
- It should be treated by urgent escharotomy (not painful as nerves are damaged).
- Suffocation:
- Due to oedema in burns of the face and neck and may need urgent tracheostomy.
- Compartment syndrome: Due to oedema of the subcutaneous tissue.
- Delayed (late) local complications:
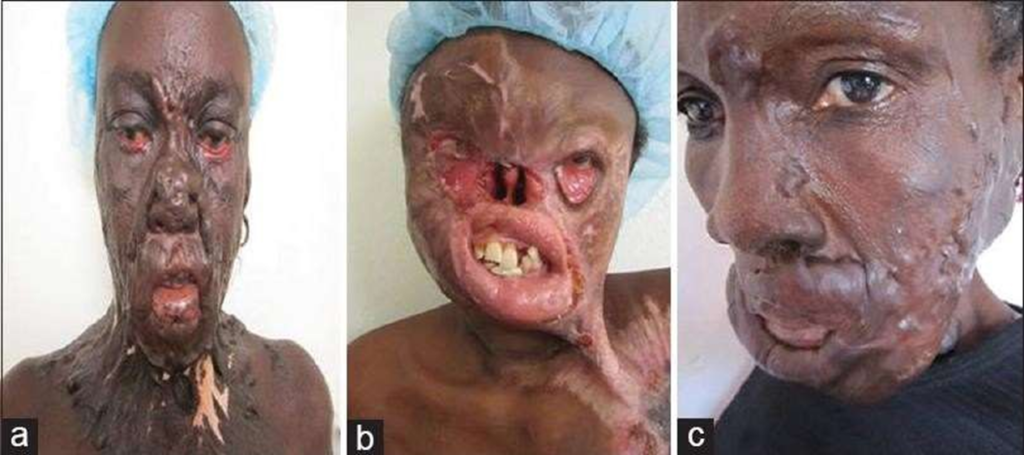
- Scarring and loss of quality of skin→ disfigurement.
- Presence of raw skin areas due to 3rd degree burns.
- Pigmentary skin changes in the form of hvpo/hvper-pigmentation
- Contractures: across joints.
- Scar formation: (hypertrophic or keloid)
- Malignant transformation (rare): (Marjolin’s ulcer) in long-standing unstable scar

Indicated in pt with burn more than 15-20%TBSA in adult and >10% in children.
Initially should established good I.V line, if not possible →Venous cutdown Foley’s catheter should be used to assess urine output
DAY 1:(Hr 0-24)
Parkland formula: most commonly used formula in first 24 hours post burn.
4cc/kg/%burn=totalvolume for 24 hr
Give ½ of total volume in 1st 8hr (from time of injury)
Give ½ of total volume in 2nd 16 hr
Use lactated ringer solution
Fluid administrationshould be titrated to urine output of 30cc/hr for adults and
1 cc/kg/hr for children.
Colloid is typically not used until 12 to 24 hours following bum injury when the capillary leak has started to seal
• What do you need to know for the burned patient to calculate fluid requirement according to parkland formula?

Background pain :Best treated with longer acting agents :MORPHIN
Procedural pain occurs during daily wound care and therapy. shorter acting agents are probably best. use of short-acting benzodiazepines is favorable
5,6,7-
Routine tetanus prophylaxis is employed.
- There is no role for prophylactic systemic antibiotic therapy. Give antibiotics when there are features of infections.
- Put NG tube and prescribe antacids :When the burn surface area is 25% or more of deep burn, the patient is liable to develop paralytic ileus and stress gastro-dudenal erosions or ulcers→ put NG tube and prescribe antacids.
8
Frequent checking of PCV, S.electrolytes, and renal function tests.

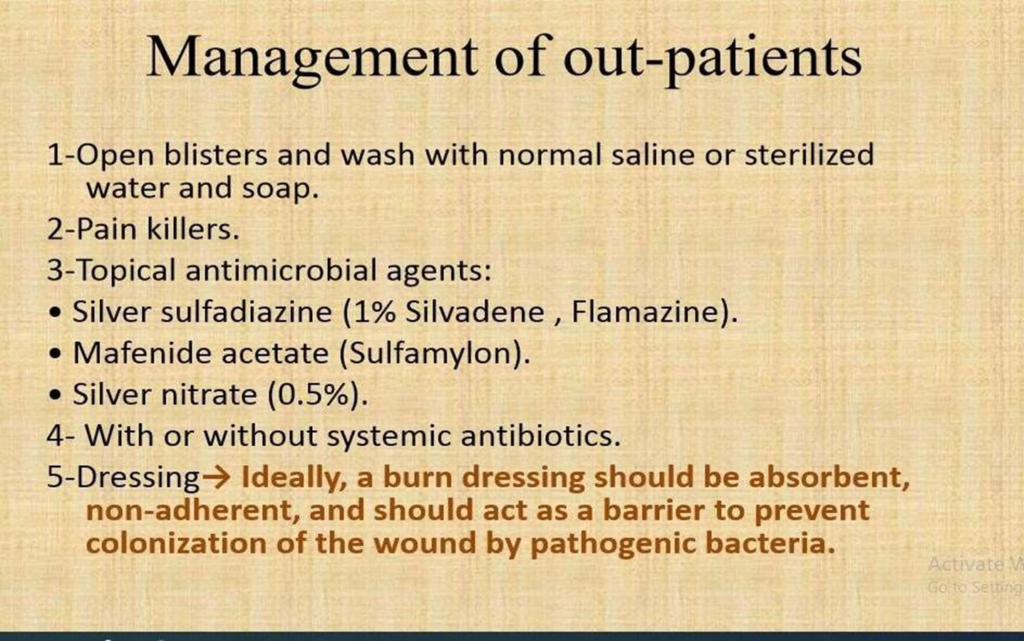
blisters are debrided. Body and facial hair are shaved if involved in the area of a burn.
Daily wound care is performed on a shower table with soap and tap water.
Use of topical antibiotic:
Silver sulfadiazine:
Mafenide (Sulfamylon
Silver nitrate(0.5%)
Bacitracin, neomycin, and polymyxin B
Povidone iodine

11. Psychlogical support. 12.Rehabilitation and physiotherapy.

- Deep dermal and full thickness burns are inelastic.
- Can cause distal limb ischemia if circumferential .
- Similarly, extensive involvement of the chest (or abdomen in
a child) can impair ventilation.
- Constriction becomes worse once fluid resuscitation is begun.
- Escharotomy relieves this constriction.
- Usually done with electrocautery, because they tend to bleed.
- Fasciotomies usually required only for burns involving muscle, or high-voltage electrical injuries.




- Early staged excision should begin on postburn day 3 in full thickness burn.
- Type of excision:

Tangential excision: sequential removal of layers of eschar and necrotic tissue until a layer of viable, bleeding tissue.granulation tissue دحل لصونم لل
Fascial excision: excision of the burned tissue and subcutaneous tissue down to the layer of the muscle fascia
Water jet-powered VersaJet: useful for excision of concave surfaces of the hand and feet, as well as for excision of the eyelids, ear, and nose




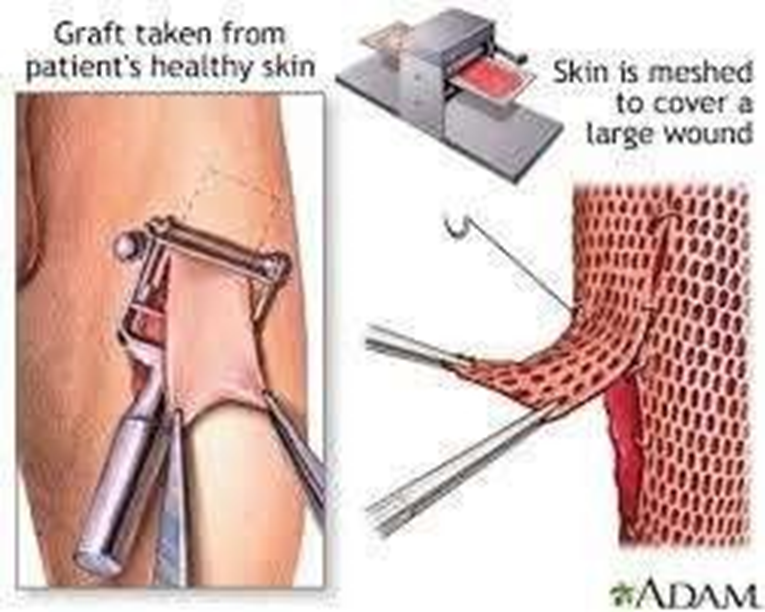
Skin graft: segment of tissue that transfer from one site of body (donor site) to another site (recipient site) without its blood supply
Types :1. Full thickness skin graft: which consist of
epidermis and full thickness of dermis.
2. Split thickness skin graft: Which consist of epidermis and variable portion of dermis, it described as thin, intermediate, and thick according to thickness of included dermis.
- Skin substitutes: in cases of extensive burn wounds, the surface area burned may exceed the available donor sites , so they need for a replacement for human skin until complete coverage with autografts can occur



Pathogenesis:
CO inhalation: CO affinity for Hb is 210 times that of O2 leading to displacement of O2
(major pathogenic affect)
Direct injury to upper aerodigestive tract
Inhalation of product of combustion(most common and significant component of
inhalational injury)
Aldehydes , keton and organic acid are produced from combustion of synthetic materials and causes significant chemical injury of respiratory tract
Diagnosis:
Presentation: Flame burn occurring in closed spaces , singed nasal hairs , facial burn , production of carbonaceous sputum . these non specific.
Sign of upper respiratory obstruction (stridor)
Arterial bloodgase analysis: determine CarboxyHb level .if >10% are significant for CO
inhalation
Fiberoptic bronchoscopy: mainstay in DX
X-Ray usually of little help unless there is other pathology
Management:
The Tx of inhalational injury is only supportive.
Airway maintenance : Patients with signs and symptoms of inhalation injury
may require intubation.
100% O2 is given if CO poison is present. The half-life of carboxyhemoglobin on 100% oxygen is 40 minutes while in room air is 250 minutes.
Aggressive pulmonary toilet, bronchodilators, and clearing of secretions .
Steroids have not been shown to be beneficial in the treatment of inhalation
injury, and the use of prophylactic antibiotics should be avoided.
Repeat bronchoscopy can be useful in obtaining sputum samples for culture and for assistance in suctioning sloughed mucosa .

hyperbaric oxygen for patients with elevated carboxyhemoglobin levels. It reduces the half life of carbon oxide from 40 minutes on 100% Fi01 to 20 minutes.
Healing
Rate of tissue healing depends on remaining hair follicles & sweat glands
Partial thickness burns: Healing by epithelialization within 3 weeks
Full thickness burns: Separation of eschar leaving granulation tissue after 4 weeks →fibrosis & scaring
TREATMENT
THANKS
AUTHOR
DR AFRAZ SHERAZI